You will forgive me for cheating this week and singling out a country for the second time in this Substack journey. Hear me out. We talked about maternal mortality in Sierra Leone and Australia and how each tells a distinct story. We cannot - OK, I cannot - talk about maternal mortality and not mention the United States which has 50 distinct stories all of which contribute to the headline you likely already know:
The U.S. has the highest maternal mortality rate of any wealthy country. In 2023, there were 18.6 maternal deaths for every 100,000 live births in the U.S. That’s almost twice the average maternal mortality rate for countries with comparable economies. And it’s nearly the same as the U.S. rate two decades ago (18.8).
This lack of progress makes the U.S. an outlier. Between 2000 and 2023, global maternal mortality rates dropped, on average, by 40%. But in the U.S., the rate spent decades climbing. By the end of 2019, it hit 20.1 deaths per 100,000 live births. In 2021, the strain of COVID-19 on an already underperforming health system pushed that number to 32.9.
Though it has fallen since, 18.6 is still unacceptably high. Some wealthy nations have almost entirely eliminated preventable maternal deaths. The U.S. can—and must—do better.
Center for Reproductive Rights (2025)
When most people think about maternal mortality, they picture an acute clinical crisis in the delivery room like a sudden hemorrhage or an unmanageable infection. But a landmark study published a few months ago shatters this assumption. When researchers looked at deaths among pregnant and postpartum women from 2018 to 2023, they found that the leading cause of maternal death was unintentional drug overdose (5.2 deaths per 100,000 live births). Violence (defined as homicide or suicide) was the second most frequent cause at 3.9 deaths per 100,000 live births. In fact, homicides accounted for 68% of those violent deaths, and firearms were involved in about 77% of them.
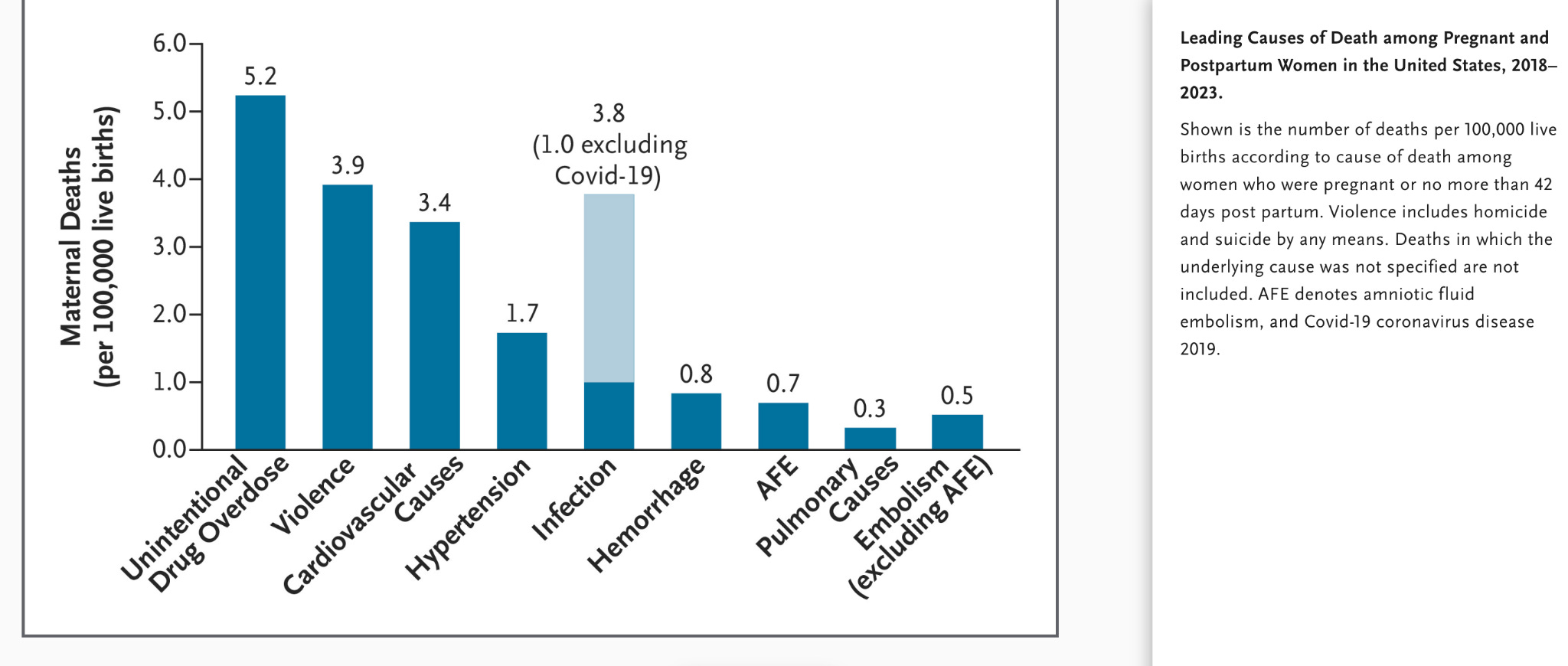
Source: NEJM (2026)
Cardiovascular causes actually ranked third. In all, violence and overdose accounted for more deaths than cardiovascular causes, hypertension, infection, and hemorrhage combined. Overdose mortality during pregnancy and the postpartum year has risen sharply alongside fentanyl penetration, embedding itself into the broader mental health crisis that is now the leading single cause of pregnancy-related death in the US.
To fix this crisis, it helps to start looking past the delivery room. Here are 5 things to know about maternal mortality in the US:
1: Native American and Black women bear the heaviest burden
As always, measurement matters. The National Vital Statistics System (NVSS) tracks maternal mortality strictly during pregnancy or within 42 days of birth (the mainstream definition of MMR). By that metric, the latest 2024 data shows an overall MMR of 17.9 deaths per 100,000 live births, and that Black women were dying at 3x higher rates than White women.
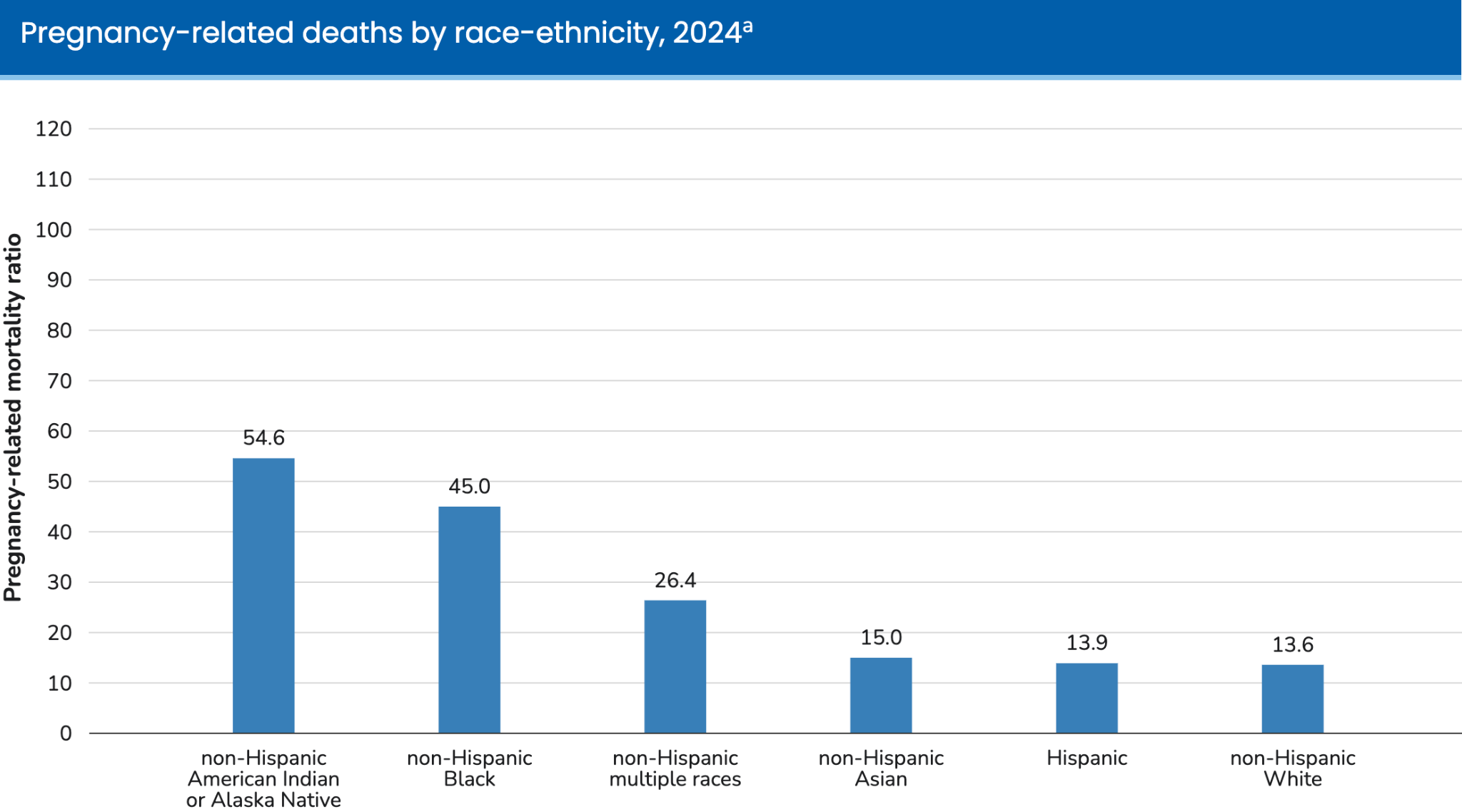
In Australia, we saw that a significant portion of deaths happen far beyond that 42 day window, into a full year post-birth. This is true in the US too, and when we switch to the Pregnancy Mortality Surveillance System (PMSS) which tracks deaths through a full year post-birth, a more complete (and devastating) picture emerges. It includes a category frequently suppressed in smaller datasets due to sample sizes: American Indian or Alaska Native (AI/AN) women.
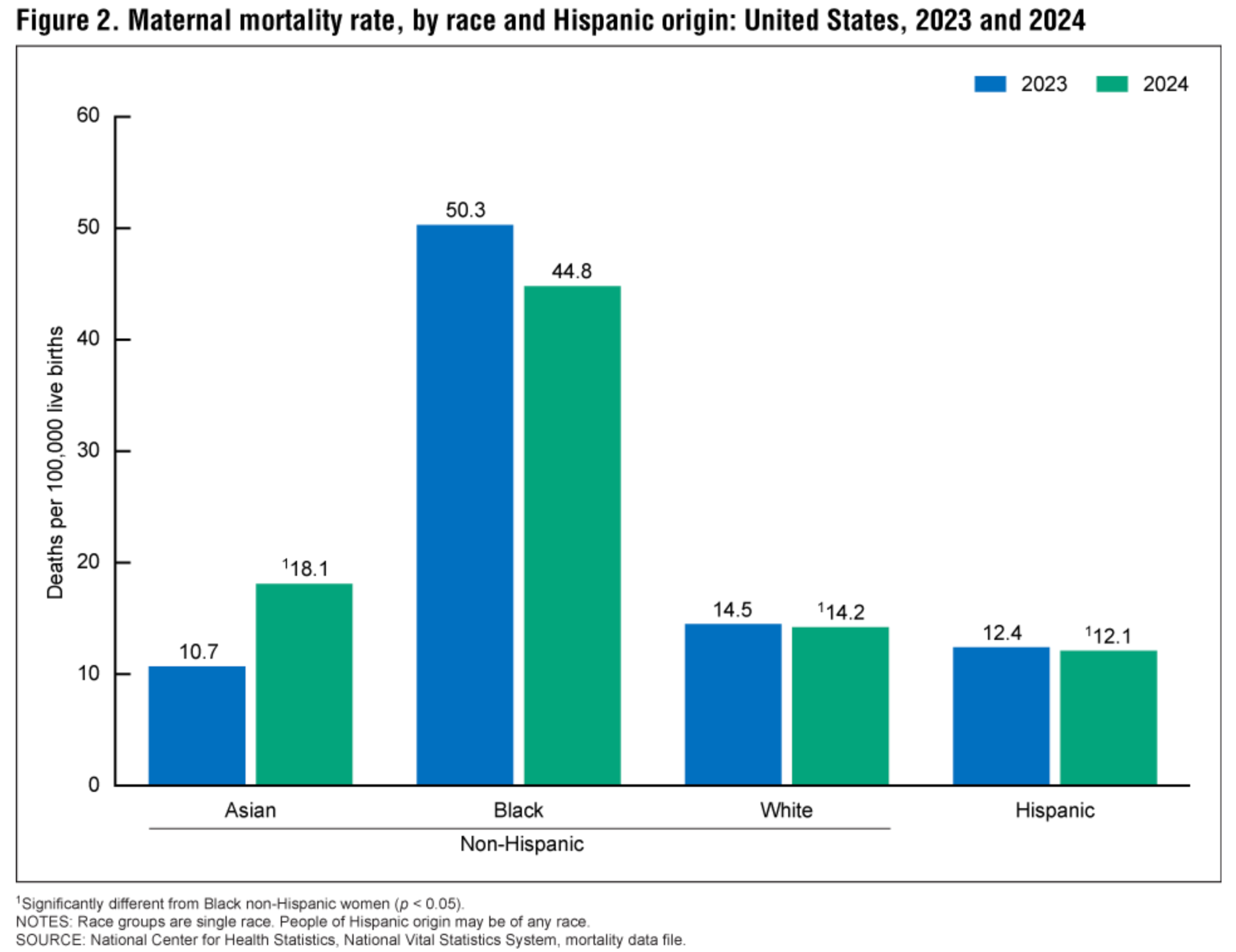
Source: NCHS 2026
Source: PMSS (2025)
Astoundingly, the full-year data shows that AI/AN women actually have the highest mortality rate in the country, about 4x that of white women, and Black women following closely at 3.3x. While there is a vital national conversation around the Black maternal health crisis, the parallel crisis facing indigenous communities is often left in the shadows. Or perhaps that’s my own gap in knowledge, I confess.
Both groups face high baseline rates of chronic conditions like obesity and hypertension, but underlying structural roots vary.
To explore these disparities further, the CDC offers an interactive portal that breaks down maternal mortality data by demographic. For instance, the leading clinical causes of maternal death vary notably by race:
Asian: Infection
Black: Cardiovascular conditions
AI/AN, Hispanic, White: Mental health conditions
While these clinical conditions account for the majority of deaths, they are almost entirely preventable. The true culprits are often the underlying systemic barriers and non-medical pain points that turn otherwise manageable complications into fatal outcomes.
For AI/AN women: There’s a lot to dig into, you can read this great summary if you have time. A few points that jumped out at me: severe geographic barriers are a dominant factor. A high percentage live in remote areas completely detached from emergency obstetric care (sound familiar - we saw this in Australia too), compounded by severe underfunding of the Indian Health Service (IHS). There is also a deep legacy of historical trauma and medical mistrust born from past institutional injustices (including forced sterilizations), making women hesitate to seek care early.
For Black women: Leading clinical causes of death include excessive postpartum bleeding, infections, and cardiovascular conditions like cardiomyopathy, with more than half of all fatalities occurring between one week and one year after delivery. However, research emphasizes that the roots of this disparity extend far beyond clinical factors. Black women experience higher rates of severe maternal morbidity and late or entirely absent prenatal care due to a combination of systemic hurdles, including limited access to obstetric providers, structural racism, and a higher allostatic load (the cumulative physiological wear-and-tear of chronic stressors and discrimination). Additionally, explicit and implicit bias among healthcare professionals frequently leads to the dismissal of Black patients’ reported symptoms, resulting in dangerous diagnostic delays. If you are looking for a beautifully done all encompassing deep-dive on black maternal mortality, I thought this was top notch.
The national divide is not an abstract average; it plays out with devastating precision in the states struggling the most.
2: Each of the 50 states could tell 50 different stories on maternal mortality
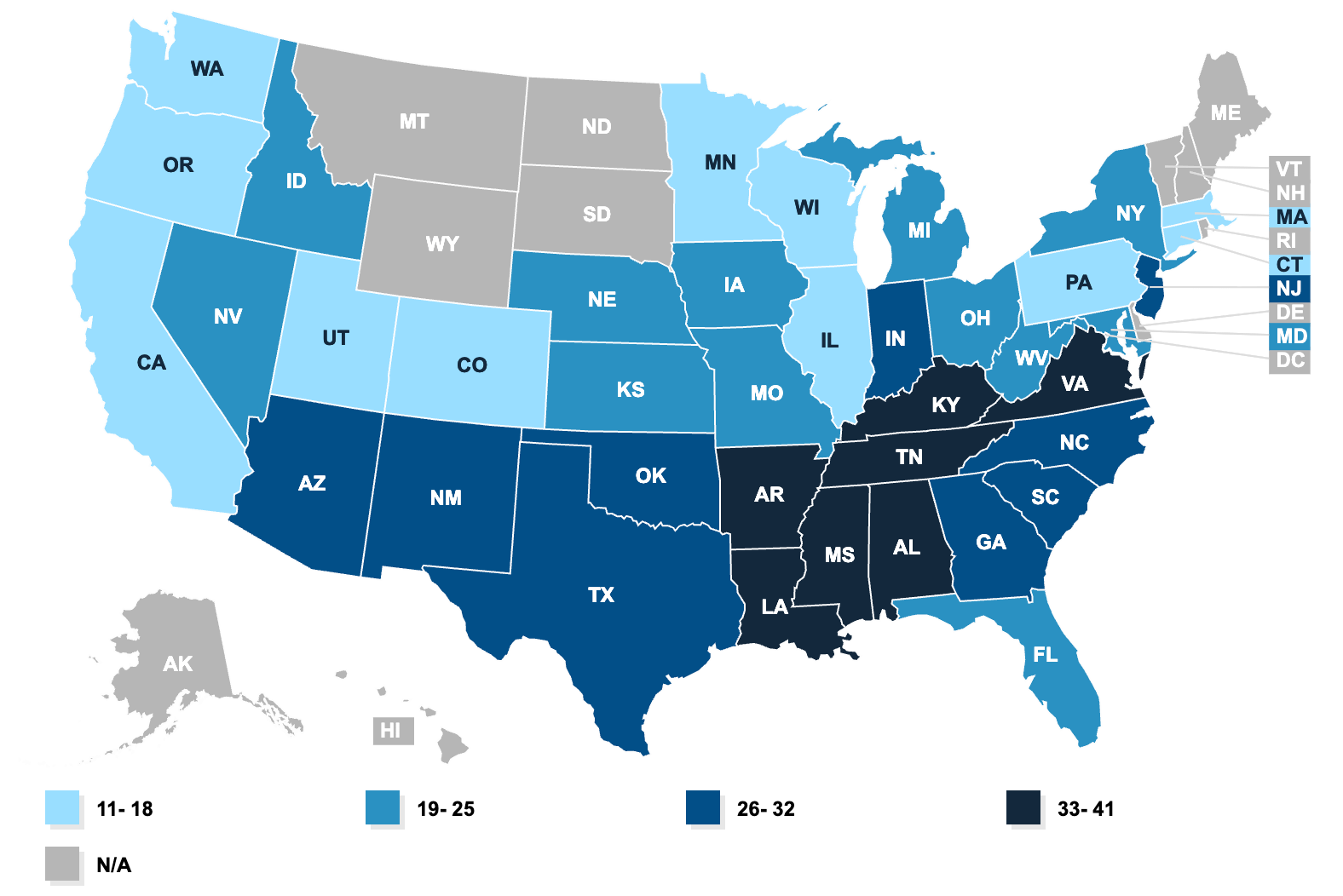
Ok, a bit of an exaggeration, but there are at least a few. According to the most recent NVSS data, the 5 states with the highest maternal mortality are: Tennessee (41 deaths per 100,000 live births), Mississippi (39), Alabama (39), Arkansas (38), and Louisiana (37). On the other end are California (11), Minnesota (12), Wisconsin (13), Utah (16), and Connecticut (16).
Source: KFF
A pregnant woman in Tennessee is nearly 4X more likely to die than a woman in California. What gives?
California significantly lowered its maternal mortality rate by forming a public-private partnership called the California Maternal Quality Care Collaborative (CMQCC), which transformed how hospitals respond to childbirth emergencies. Instead of leaving emergency protocols up to individual doctors, the state analyzed real-time public health data to identify the most preventable causes of death, specifically severe bleeding (obstetric hemorrhage) and pregnancy-induced high blood pressure (preeclampsia). They developed standardized, evidence-based safety toolkits that equipped hospitals with specific checklists, emergency carts, and team drills, treating maternal emergencies with the same uniform precision as a cardiac arrest response. By scaling these protocols across nearly all of its birthing hospitals, reducing unnecessary C-sections, and bridging the gap between data collection and rapid clinical action, California managed to cut its maternal mortality rate in half while rates across the rest of the country rose.
When the Tennessee Maternal Mortality Review Committee (MMRC) released its 2025 report, it uncovered a heartbreaking statistic: the vast majority of these maternal deaths were entirely preventable. So why can’t Tennessee implement some of the things that California has? Lack of political will? Prioritization of other areas? Either way, your survival seems to depend heavily on non-clinical variables. Your zip code dictates access to prenatal care, insurance coverage, and legal protections.
It depends on:
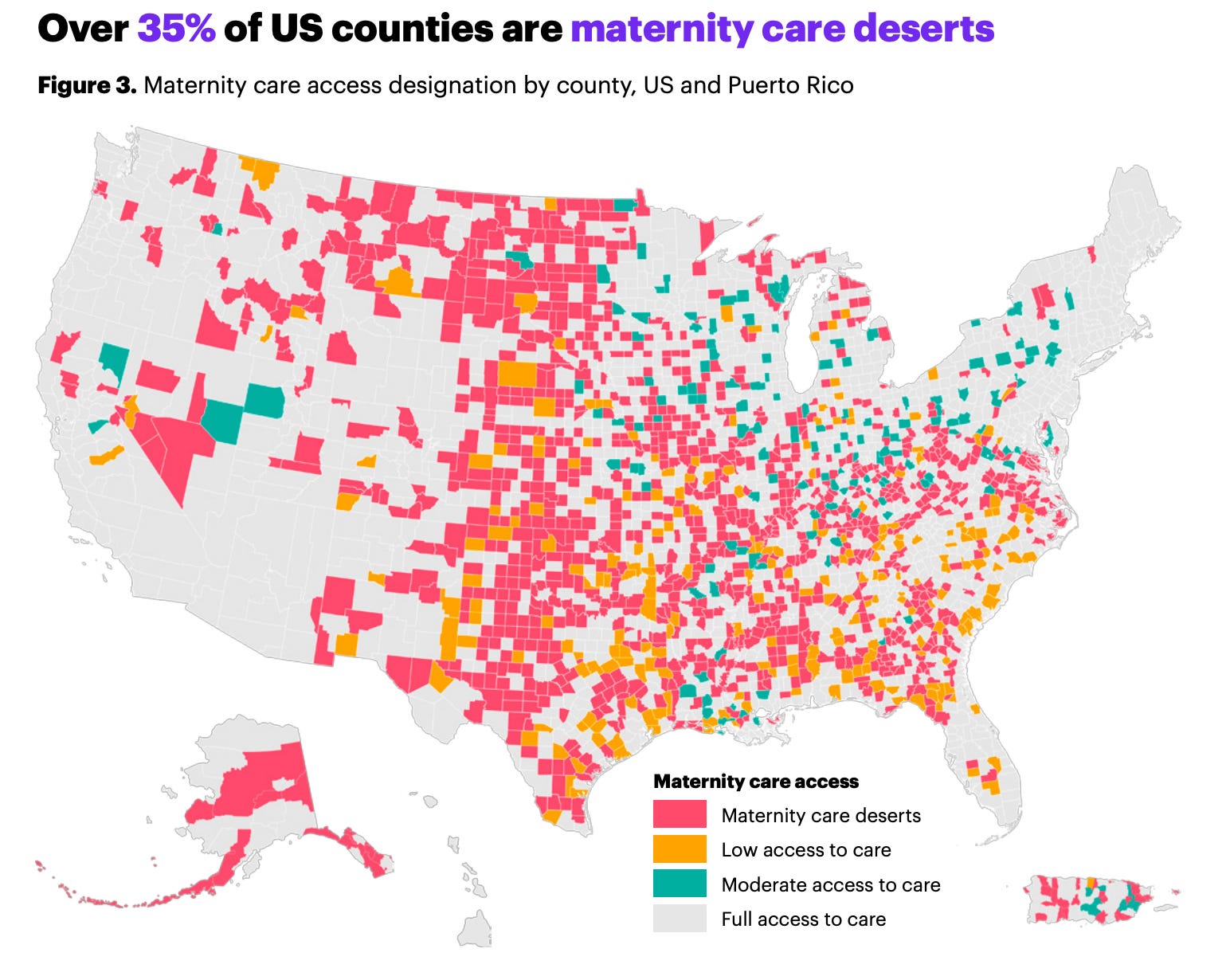
Whether you live in a maternity care desert: That’s about 35% of US counties (see map below). Maternity care deserts overlap with the regions of highest pre-pregnancy chronic disease burden. In Tennessee, rural hospital closures have gutted local access, leaving entire counties without a delivering hospital (!)
Source: March of Dimes (2024)
Whether the hospital where you delivered still has an OB unit: From 2010 to 2022, a total of 238 rural and 299 urban hospitals lost their obstetric services while only 138 hospitals, mostly in urban locations, added them. By 2022, more than half of all rural hospitals (52.4%) no longer offered obstetric care, up from 43.1% in 2010. Urban hospitals were not spared either, with 35.7% lacking obstetric services by 2022, compared to 29.7% a decade earlier
3: Insurance coverage is life-saving (but stalled by policy)
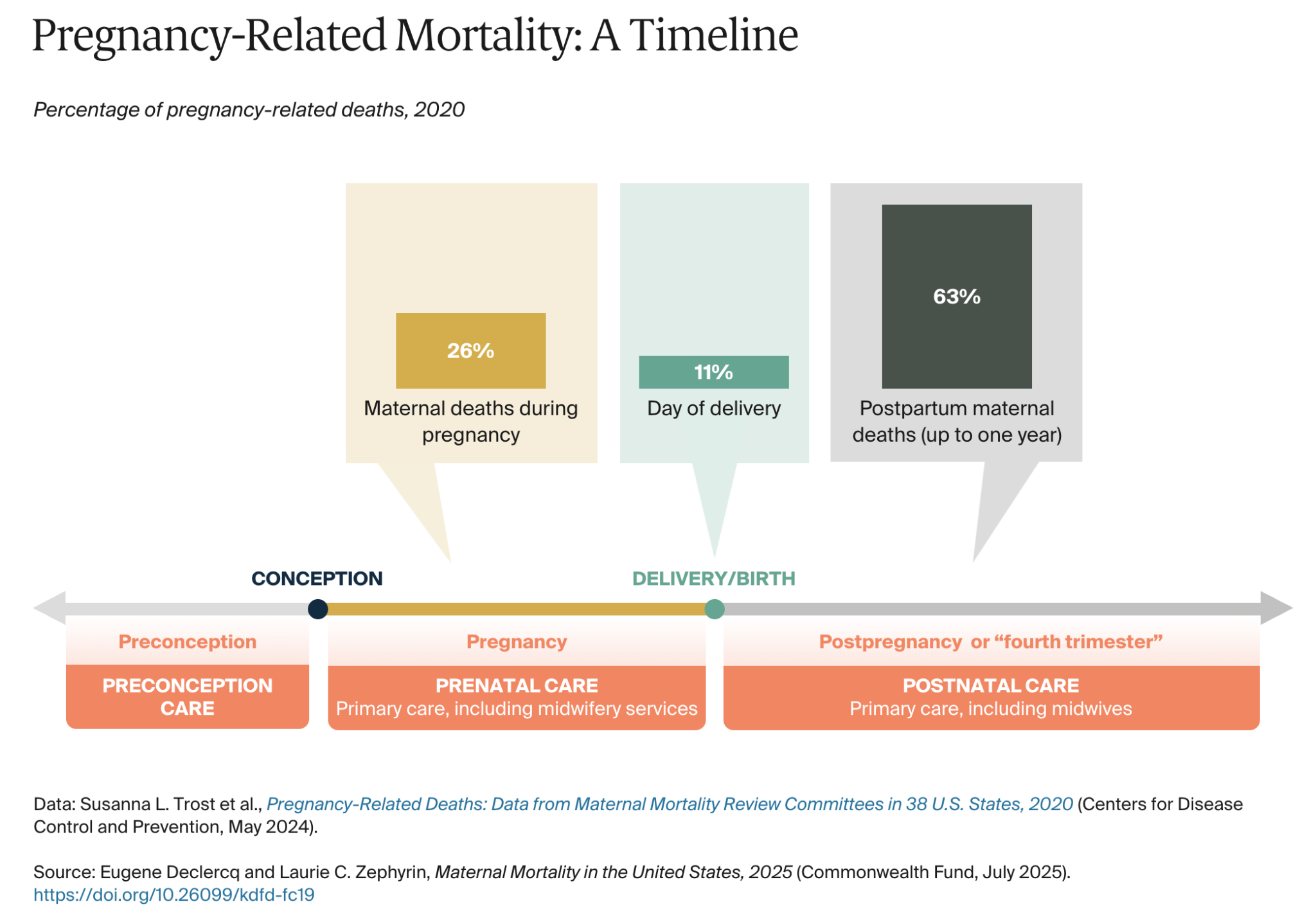
Medicaid finances roughly 40% of all births in the United States. Historically, federal law only required states to provide this pregnancy-related coverage through 60 days postpartum. But as the data shows, a majority of maternal deaths occur after that arbitrary 60-day window.
This abrupt cutoff has left new mothers exposed precisely when they are most vulnerable, rendering the 60-day limit entirely ineffective at tackling the root drivers of maternal mortality.
To bridge this gap, the American Rescue Plan Act of 2021 allowed states to extend postpartum Medicaid coverage to a full 12 months. While momentum became near-universal by early 2026, progress remains staggered, and a handful of holdouts (including Arkansas, Idaho, and Wisconsin) have kept limitations or partial proposals in place.
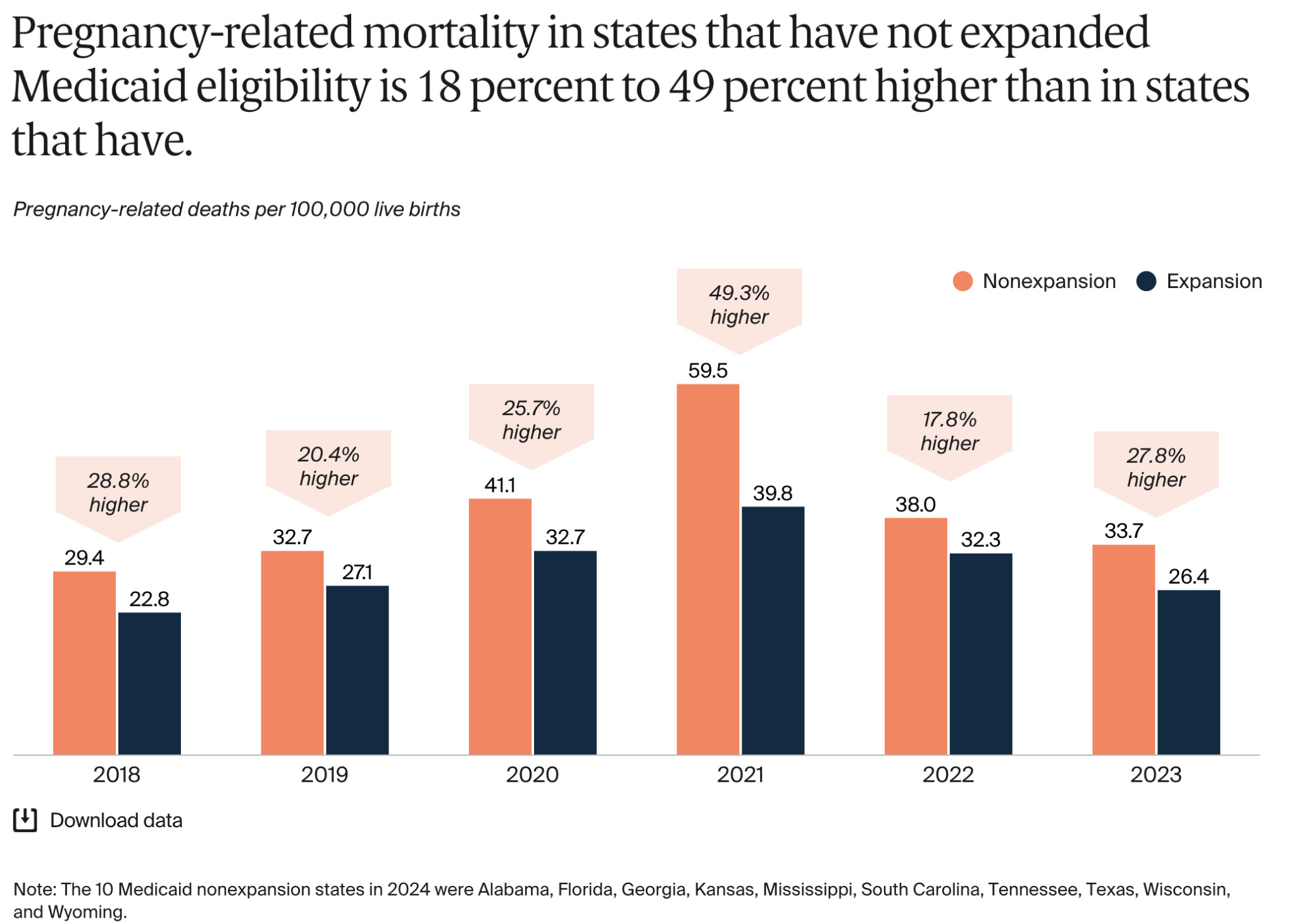
Expanding health insurance coverage, both through the broad Affordable Care Act (ACA) Medicaid expansion and the specific one-year postpartum extension is a fundamental pillar in fighting the American maternal health crisis. The data on this is stark: maternal death rates are 18% to 49% higher in states that have rejected broad Medicaid expansion compared to those that accepted it.
Historically, the Deep South has invested the least in maternal health, and the region continues to suffer from the poorest maternal and infant health outcomes in the country. Ensuring women have adequate coverage during the “fourth trimester” is the lowest-hanging fruit in policy response. A mother’s healthcare safety net should not vanish just as her postpartum mental health and cardiovascular risks peak!
4. State abortion bans and restrictions are worsening the crisis
The legal landscape is a critical analytical layer for maternal mortality particularly with respect to the geographic divide. Since the overturn of Roe v. Wade in 2022, half the U.S. states have banned or severely restricted abortion. These bans and restrictions are undermining access to reproductive care of all kinds. This includes early pregnancy care, miscarriage management, and treatment for dangerous pregnancy complications. Data compiled by the Center for Reproductive Rights (summary here) highlights how these bans undermine reproductive care of all kinds. Their impacts are many:
Doctors are leaving states with abortion bans, worsening shortages. Those who stay are being pushed to deprioritize maternal health in favor of the fetus. In serious pregnancy complications, abortion is necessary and life-saving. But many doctors now fear losing their license or facing criminal charges for providing it.
Abortion bans are also driving delays in prenatal care. Pregnant people may wait to see a doctor until after their first trimester, fearing that a miscarriage–misconstrued as an abortion—could result in criminal charges. A 2024 report also found that providers in abortion ban states are sometimes encouraging patients to delay care for the same reason These impacts are falling disproportionately on Black and Indigenous women, who are more likely to live in states with abortion bans. They are also less likely to have the resources necessary to travel out of state.
The bottom line is this: Mothers living in states that banned abortion nearly 2x as likely to die during pregnancy, childbirth, or soon after giving birth, compared to mothers living in supportive states where abortion was legal and accessible. Strikingly, post-Dobbs data reveal that maternal mortality FELL by 21% in supportive states where care remained accessible.
5: There is a great deal of innovation underway confronting the layers of challenges associated with maternal mortality in the US
There has been a recent surge in technological innovation, driven by venture capital funding and specialized healthcare accelerators to tackle the many layers of the maternal health crisis.
Recognizing that a staggering number of severe complications and pregnancy-related deaths are preventable, initiatives like Winrock international’s MaternaTech project in Arkansas is bridging the gap between emerging health-tech startups and major hospital systems. These accelerators provide capital, clinical mentorship, and pilot opportunities to rapidly scale solutions that address gaps across prenatal, perinatal, and postpartum care. The idea is to ensure that these tools are closely aligned with healthcare financing, insurance providers, and front-line clinicians to move away from the fragmented system of care that currently exists.
Serena Williams, who sadly underwent a near-death experience during childbirth herself, has backed startup Mahmee which utilizes data-driven platforms to offer personalized and on-demand support, and continuously monitor new moms up to a year after birth. Similarly, startups like Pomelo Care use proprietary digital tools to offer continuous risk-stratified engagement during pregnancy, while digital health platforms like the Maven Clinic expand comprehensive virtual care access. To tackle acute clinical crises, companies are also using targeted physical and AI innovations. For example, startups like Varda5 equips multidisciplinary teams with the skills to effectively manage maternal medical and delivery emergencies., while automated systems like BioticsAI use AI to improve fetal ultrasound screenings, and Vasowatch focuses on reducing postpartum hemorrhage risks in real time.
Crucially, this welcome wave of innovation is attempting to redefine equitable care by integrating culturally competent, community-based support directly into digital frameworks. Platforms like Mae for instance, are specifically optimizing care for Black mothers by providing digital infrastructure that connects them with local doulas and handles administrative barriers to secure insurance reimbursement. At the same time, tech forward models like Oula and blending the expertise of midwives and OB-GYNs, utilizing collaborative digital platforms to give patients agency and continuous communication throughout their journeys. I really enjoyed learning about all these different ways that life-saving interventions are accessible, continuous, and culturally attuned; potentially reshaping how maternal care is delivered in the US. That said, almost no venture-funded company is addressing the rural maternity desert: the geographic core of the US MMR problem (Mississippi Delta, Appalachia, rural Texas/Louisiana).
Looking ahead
So if venture capital hasn’t looked to fund rural clinics yet, state legislatures resist broad Medicaid expansion, and funding cuts have gutted programs responsible for monitoring maternal health, what is the alternative?
Well, I am not sure, but glimmers of hope are presented by some recent initiatives. The Rural Health Transformation Program (RHTP), spearheaded by the Centers for Medicaid and Medicare Services (CMS), represents a shift in how we approach healthcare delivery in underserved parts of the country. The RHTP includes chronic disease management, a proposed expansion of the maternal health workforce and more. Snarkily, I have to include this statistic from the KFF: Immigrant adults make up nearly three times the share of physicians and surgeons in rural America than their share of the overall rural workforce (14% vs. 5%). This expansion should be interesting to watch, with a lot of confusion and panic over visa statuses. While $50 billion is better than nothing for rural health communities in America, it will never be able to offset the $900+ billion in Medicaid cuts that was also a result of the same Bill that funded this (ahem, the “One Big Beautiful Bill”). For a state like Tennessee, leveraging the RHTP isn’t just a policy option; it is the blueprint required to keep rural hospital doors open and stop the geographic lottery that dictates whether an American mother lives or dies.
That said, we cannot purely innovate our way out of this crisis with bespoke apps and platforms for the affluent. Nor can we wrangle our way out of it if we simultaneously allow rural hospital infrastructure to crumble or gut the funding required for state committees to monitor their data. To fix the crisis, we must start addressing the structural and demographic map of where American women are actually being left behind.
The Food!
Cardiovascular risk aside, we decided to make something from our top MMR state, Tennessee. This all sounds so rude, but go with it. I was discusing this with my friend Madeleine, who is not only from Nashville, but whose mother Nancy has a cookbook! I used her awesome recipe to make Nashville Hot Chicken. We ate that deliciousness with vinegary coleslaw, pickles, and mac and cheese. We took this opportunity to sing along to all the Dolly Parton songs, and of course, Zac Brown Band’s Chicken Fried.