

Australia is one of the safest places in the world to give birth, globally recognized for its exceptional standards of healthcare. Maternal death is a rare event. This is in stark contrast from last week’s case study, Sierra Leone, where maternal mortality remains a public health crisis, although undergoing impressive improvements. That said, the context of maternal death in Australia, when it does occur, is due to very different reasons with very different implications. Which is why I decided to focus on the reasons behind maternal mortality in a country like Australia, instead of focusing solely on what they are doing that’s awesome. It’s a story that I think is more urgent for right now.
In Sierra Leone, maternal mortality is a crisis of biological youth, economic underdevelopment, and acute infrastructural deficits. In Australia, it is related to a different aspect of demography (fertility postponement, advanced maternal age, and a rising profile of non-communicable chronic diseases) layered over geographic vastness and systemic equity gaps.
But first, a little bit about Australia’s population story. And because it did come up in my search, I must tell you that indeed, there are more kangaroos than humans in the country with a 1.36:1 ratio. You are welcome. There’s currently about 27 million people in the country, with a nifty population clock to boot, and a median age of about 38. Australia has a rich mix of cultural backgrounds and heritage, with the number of people living in Australia who were born overseas continuing to increase (currently at 32%) with India, England, China, and New Zealand leading the countries of origin. First Nations (Aboriginal and Torres Strait Islander) communities make up 3.5% of the total population, with 92% of the group identifying as aboriginal.
What’s happening with maternal mortality?
In 2023, the most recent year for which data are available, there were 23 maternal deaths nationwide. This represents a maternal mortality ratio (MMR) of 8.2 deaths per 100,000 women giving birth, an increase from the previous year. BUT, due to the small number of maternal deaths in a year, it can be difficult to interpret the trend in maternal mortality over time using single year rates. Australia uses a triennia approach (aggregating three years of data) to get around that.
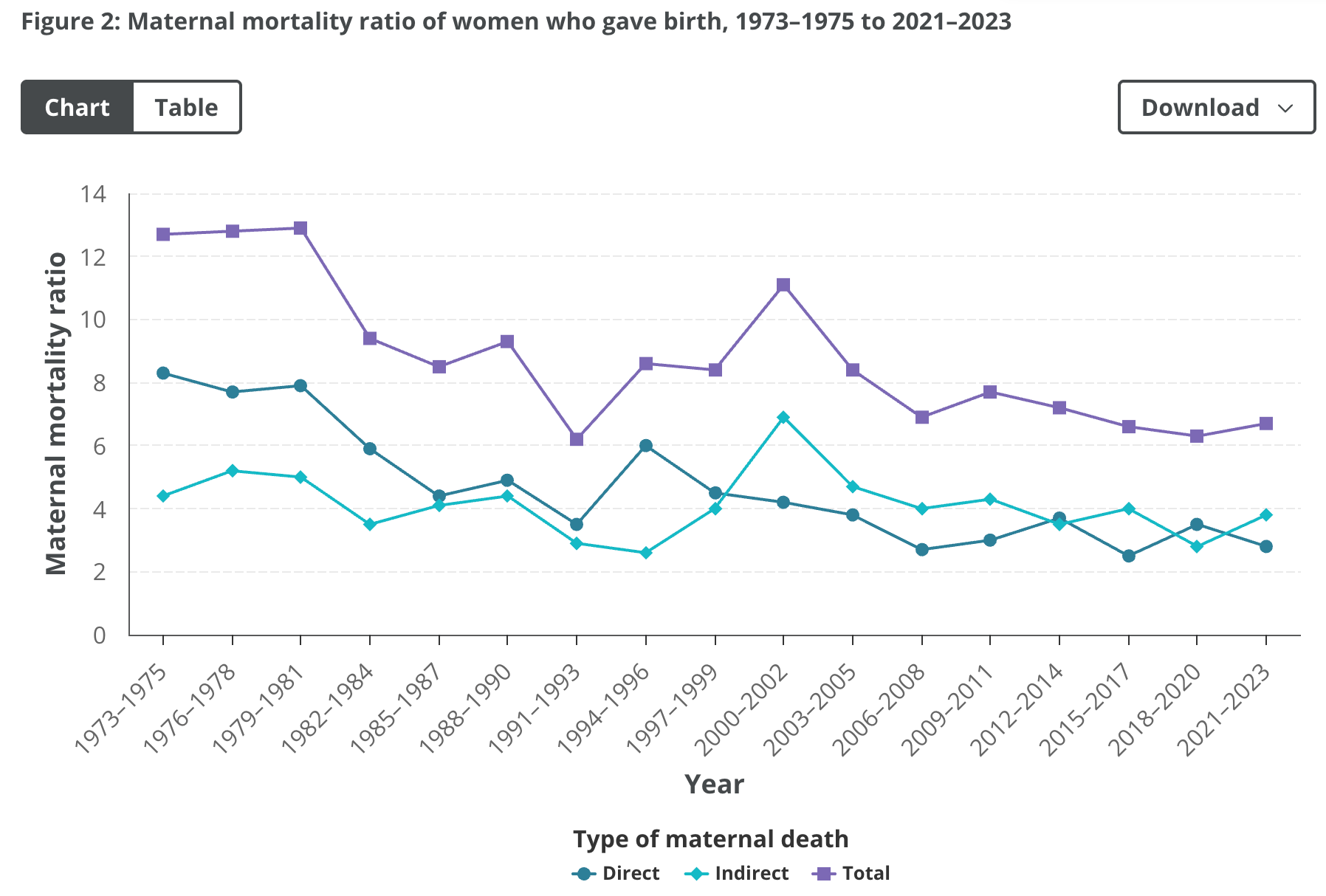
Source: Australian Institute of Health and Welfare (2025)
Over the past 50 years, the rate has fluctuated at times but overall the MMR has declined, from 12.7 in 1973–1975 to 6.7 per 100,000 women giving birth today. It’s important here to point out that the MMR for First Nations women is more than 3X that of non-indigenous women, due to a variety of documented reasons:
Racism and lack of cultural safety in hospitals and from healthcare providers
Pregnant First Nations women avoiding antenatal care for fear of child protection services taking their children. This is a legacy of the “stolen generations” with continuing high rates of child removals
Closures of regional and remote birthing services requiring more First Nations women to leave home and travel long distances to give birth, often alone. Some women opt to give birth without a midwife, which can have significant issues for mother and baby.
The leading causes of all maternal deaths in Australia between 2014 and 2023 were cardiovascular disease, sepsis, suicide and thromboembolism (below):
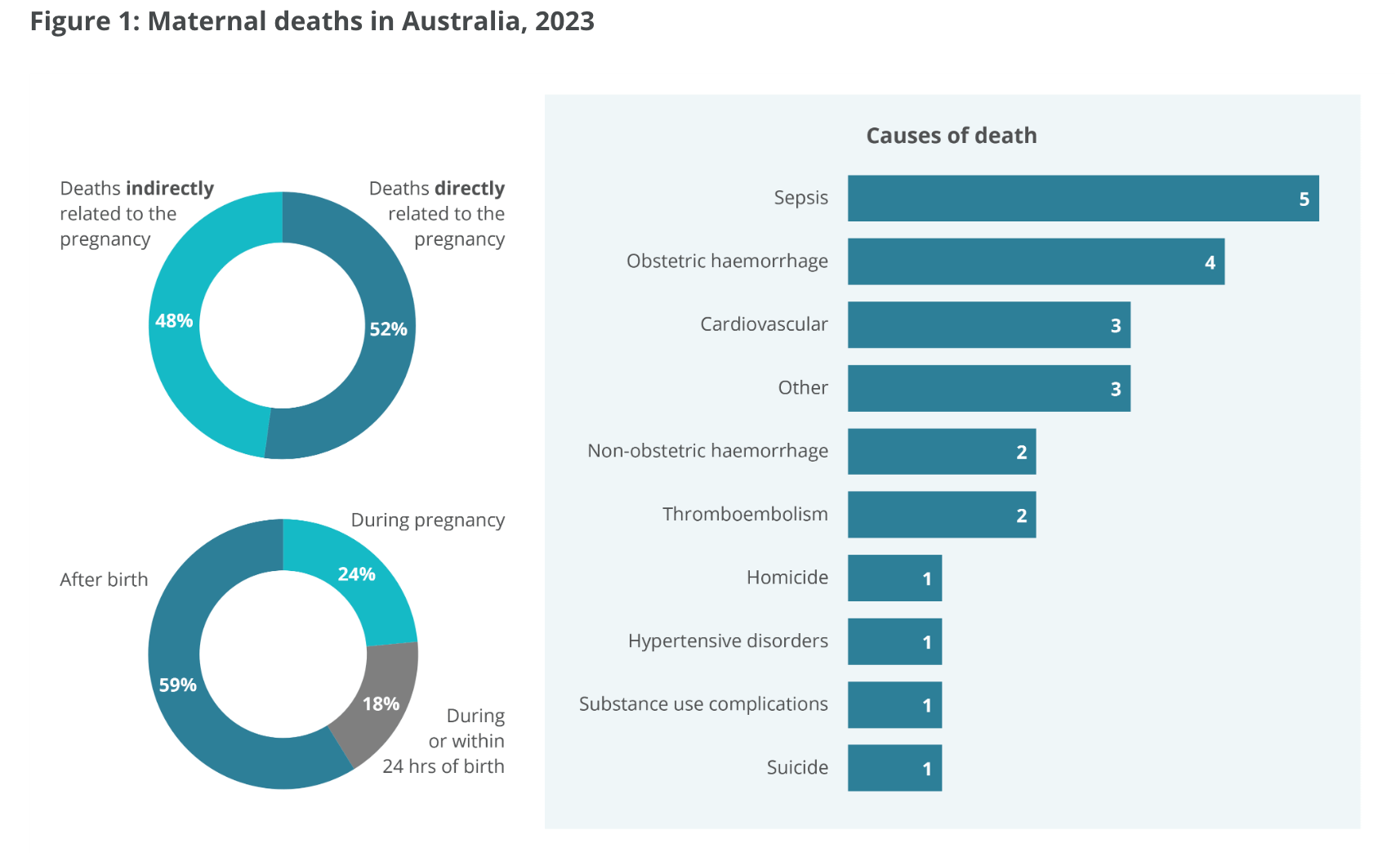
Source: Australian Institute of Health and Welfare (2025)
However, recent evidence shows that these structural disparities can be directly addressed.
Implementing culturally specific and tailored midwifery caseload models, such as the Baggarrook Yurrongi program and Birthing on Country initiatives, dramatically improves safety outcomes. When First Nations mothers receive continuous care from a known midwife in a framework co-designed with Aboriginal Community Controlled Health Organisations, they report feeling emotionally and clinically safe. This tailored approach has been shown to increase attendance at antenatal visits, reduce premature births by up to 38%, and significantly lower instances of infant trauma.
Maternal Age + Complications
Going back to the leading causes of death - while the first two leading causes of death are not shocking, I was surprised to see cardiovascular disease as a standalone (at 14% of all maternal deaths). To dig into that, it helps to start with one more data point: the mean age at birth. There is this evidence-based understanding that maternal mortality and age have a “J” shaped relationship. Essentially, the risk of death is high for adolescents (15-19) compared to those 20-24, and then the risk goes down, only to go up again at age 30+.
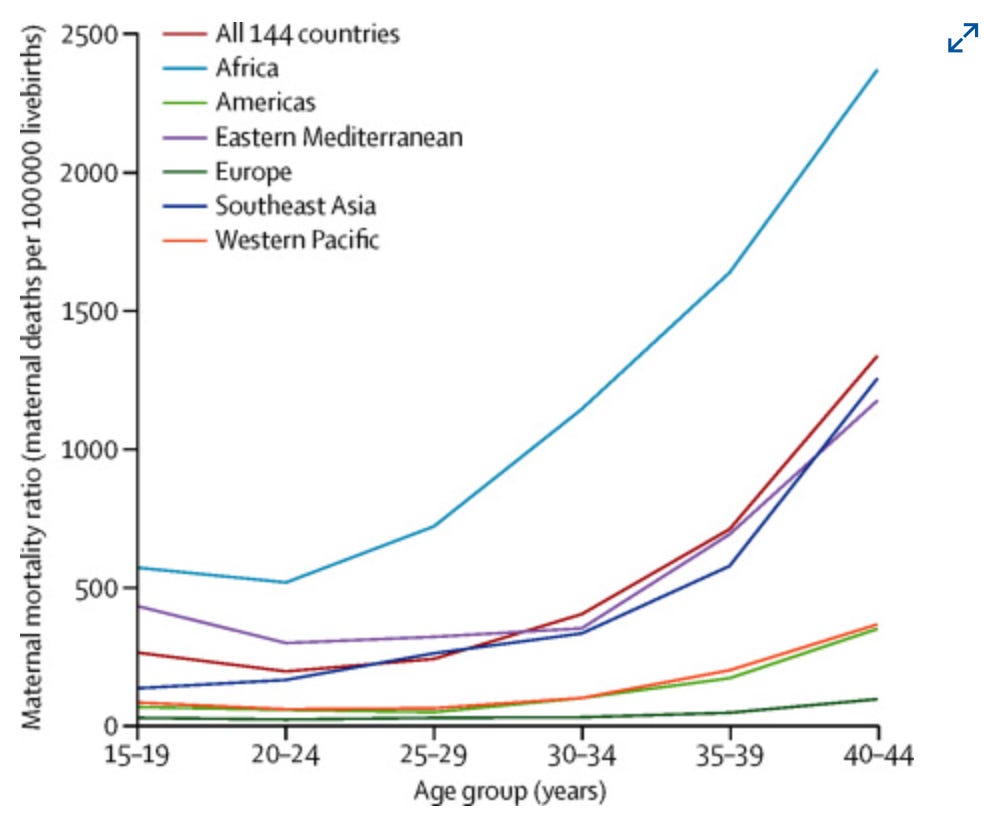
Source: Lancet (2014)
So think about Sierra Leone, where adolescent fertility is high as is the MMR. In fact, I did not underscore this point last week, but adolescent girls (age 10-19) account for approximately 20–40% of all maternal deaths in the country. [The reasons are a mix of biological immaturity and intense social vulnerability, I explored this a little in South Sudan and other posts if you recall.] In Australia too, women aged under 20 had the highest MMR, followed by those aged 40 or more (19.2 and 14.8 per 100,000 women giving birth, respectively). For older women, the risk of maternal death is linked to biology and pre-existing chronic conditions, including cardiovascular disease, hypertension, diabetes, obesity etc. Indeed, across most high-income nations including Australia, cardiac disease has steadily emerged as a leading cause of maternal mortality, heavily driven by shifting demographics, advancing maternal age, and a rising profile of cardiovascular risk factors among pregnant individuals.
The overall story in Australia is that the average age of women who gave birth has steadily increased (28.9 years in 1998 to 31.3 in 2023). In 1999, only about 14% of births were to mothers aged 35 or older. By 2023, 25% (1 in 4) of all women giving birth in Australia were 35 or older. Non-Indigenous mothers are more than twice as likely to give birth at age 40 or over (4.6%) compared to First Nations mothers (2.0%). The reasons for this postponement of fertility or advancement in maternal age are many, recall the South Korea exploration a few weeks ago. These include delayed marriage, career pathways, financial factors. In countries like Australia, certainly access to Assisted Reproductive Technologies like IVF could substantially affect the extent to which childbearing delay will be compensated at older ages.
But this also means that pre-existing conditions may be exacerbated:
The relative risk of pregnancy-related cardiovascular complications do not increase with maternal age, suggesting that aging does not substantially drive pregnancy-specific mechanisms of cardiovascular events. Rather, it appears that pregnancy uniformly heightens patients’ baseline risk, resulting in more cardiovascular complications in older patients who have higher cardiovascular risk to begin with than younger patients.
Nature 2026
The solution then isn’t to pathologize older mothers, but rather to shift traditional obstetric care toward screening and managing pre-existing, non-communicable conditions (obesity, hypertension, cardiovascular health) earlier. As fertility postponement is reality in Australia and honestly, in half the world, the conversation really needs to shift from “how can we make women have more babies,” to “how can we make childbearing safer?” To say nothing of how to make it affordable/easier to raise said children. Topic for another day. In short - traditional obstetric models need to be better equipped to screen and manage newer vulnerability profiles.
Postpartum Mental Health
In Australia, the ‘traditional’ causes of maternal death (haemorrhage, hypertension, pulmonary emboli and sepsis) are now low. However, deaths following psychiatric and medical causes persist, often beyond the standard postnatal definition of 42 days. This bears out in the MMR data, where suicide accounts for 10% of all maternal deaths in the country. It’s likely even higher because that timeframe (42 days) is insufficient for capturing the true scale of the maternal mental health crisis; if Late Maternal Deaths are counted (This refers to the death of a woman from direct or indirect obstetric causes more than 42 days but less than one year after termination of pregnancy), then suicide would be the leading case of maternal death in Australia.
A systematic review of the linkages between suicide and maternal mortality find that risk factors for suicide and suicidal ideation in the perinatal (pregnancy and 1st year) are multifaceted. They include prior mental health conditions, depression, other psychiatric disorders; poor sleep quality and emotional dysregulation; substance use; history of trauma and abuse, intimate partner violence; and socioeconomic and demographic factors (age, social and financial vulnerability)
Importantly, the authors emphasize that the widely held belief that pregnancy and the postpartum period inherently protect against suicide risk may be inflated, making it critical for clinicians to remain vigilant, particularly for patients with existing mental health diagnoses or a history of suicide attempts. Ultimately, because the perinatal period involves increased contact with medical professionals, implementing universal screening for suicide alongside depression and anxiety, combined with expanding access to mental health care, offers a vital opportunity for life-saving interventions.
In Australia, there is a helpline called PANDA (Perinatal Anxiety & Depression Australia National Helpline), which offers support to callers impacted by emotional health challenges in the perinatal period. Callers receive counselling from professional staff and peer support from volunteers. Research looking at the reasons for caller distress are complex, and include: stressful life events; pregnancy, birthing and parenting experiences; social isolation; and histories of mental health difficulties. That bit about isolation really stood out to me; parenting can be a really isolating experience for many, particularly first-time parents. There are some great organizations that have stepped in to help, Motherland came up as a lovely example. Here is a statement from the founder:
Motherland is a national charity improving the mental health of rural mothers by reducing isolation and increasing access to support — no matter where they live.It takes a village to raise a child, but for many women living rurally, that village simply doesn’t exist. Social isolation is one of the biggest challenges facing rural mothers and is a known risk factor for poor mental health. Across Australia, mums in the bush are struggling; often without access to the support networks and services many others take for granted. After experiencing crippling isolation and my own mental health challenges following the birth of my children, I became fiercely passionate about ensuring no rural mum feels alone in her motherhood journey. Motherland exists to ensure no rural mum is left behind. We deliver programs and services that reduce isolation and improve mental health outcomes, including the Motherland podcast, our online Motherland Village program, Scholarship Fund, Motherland Connect platform, national support network, events, and advocacy.
The need is urgent. At least 50% of rural mums say they can’t access a mother’s group, and more than 80% say isolation is the hardest part of rural motherhood. Without connection, the risks to mental health are significant — but with the right support, outcomes can change. Motherland has already connected thousands of rural women across the country, creating a powerful, accessible support network where it’s needed most. Because every mum deserves a village…no matter where she lives.

Source: Motherland Impact Statement (2025)
Rurality and Highway births
The point above about rural isolation and maternal health (and likely health outcomes more generally) is fascinating from a demographic lens. Remember way back when in weeks 3 and 4 we talked about the urban/rural continuum (Singapore and Papua New Guinea)? Essentially, the world is becoming more and more urban. BUT, there are significant rural populations in some countries that are not only rural, but really spread out. The population density ratio (people per sq km of land) is very low in Australia, at about 3. Other high income countries are about 27, Singapore is 8,242 and PNG is 23. But unlike PNG which is teeny tiny in terms of size, Australia is massive.
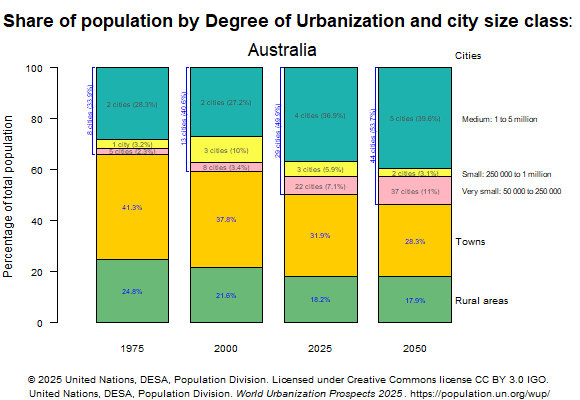
Source: World Urbanization Prospects (2025)
So while the population in rural areas and towns is declining, it is still half the current population in the country and is quite spread out. Since the 1990s, Australia has closed approximately 50% of its rural maternity services, creating vast maternity deserts. The reasons range from workforce shortages, safety and quality concerns, and cost considerations; likely related to the declining rural populations and perceived reduced need for services. What this effectively means though, is that you may be in transit to a far away hospital when you need to be delivering in comfort under medical supervision. You can guess what’s next: birthing on the side of the road (and some not making it):
“Women should not be forced to birth their babies on the gravel on the side of the road due to lack of investments in maternity and emergency care throughout rural hospitals in Australia”, said Alecia Staines, Founder of Maternity Consumer Network.
With increasing roadside birth rates, some almost 1 in 50 births, they are wanting to see local maternity services, emergency care, more midwifery access and improved outcomes for country women and their babies.
Additionally, antenatal care visits may be lower due to the added hassle of getting to a hospital for regular check ups, which then may miss the critical points of intervention should there be a mental health crisis.
Looking ahead
So while women in Sierra Leone face bad roads, infrastructure, and climate crises that delay reaching hospitals, women in Australia may just live too far away because their local hospitals have been shuttered. Australia is one of the most highly urbanized nations, yet its vast landmass creates a hyper-concentration of services in urban coastal hubs. When regional clinics close due to urban-centric economic modeling or staffing shortages, it transforms rural geography into a clinical hazard. Additionally, I wonder if a lack of local/regional options may drive more women toward unassisted home births or even “freebirthing,” which do carry clinical and legal risks (currently only about 3% of births in the country).
Whether a mother is stranded on a flooded, unpaved road in West Africa or driving down a dark, empty highway in the Australian Outback, a common failure is one of infrastructure and imagination. We cannot solve modern demographic shifts with legacy obstetric models. If half the world is going to continue postponing childbearing as reality dictates, the policy conversation must shift entirely. We must stop asking how to incentivize women to have more babies, and start building systems that make childbearing safer, integrated, and supported at any age, in any zipcode.
Innovative, community-led frameworks offer a clear path forward as seen with the examples of midwifery models for First Nations women or Motherland for rural women. It still takes a village to raise a child, and more importantly, to support a mother. But as our global population dynamics evolve, we must recognize that the village can no longer be taken for granted. We have to actively fund it, design it, and protect it.
The Food!
Don’t laugh, but we really wanted to incorporate vegemite into our Australian feast, so ended up making breakfast for dinner. We made soft-boiled eggs with avocado toast, sauteed mushrooms, baked beans, (very burnt) bacon, and a lovely salad. All eaten on sourdough with dollops of butter and vegemite. It was an unexpected hit. Of course, we ended with Tim Tams. No one did research - everyone was struggling to just make it through this week. We started out listening to Kylie Minogue and then switched to the Spotify aboriginal music playlist. We made it through the week, y’all, hope you did too!
