I’m going rogue this week. Instead of debuting a new twin pairing, I am sticking with the under-five mortality rate (U5MR). I felt a little unsettled with the unfair comparison between South Sudan and Estonia in the last 2 weeks. I know, I know: by design, for this Substack I choose countries at extreme ends of demographic indicators to investigate the guardrails of what’s possible. The idea is to show the how (structural mechanics of survival when a trend is pushed to a limit) to understand the why (motivations, constraints that drive the data). Still, this last pairing felt egregious for its mismatch- of course things would be better in South Sudan if they had the resources, stability, and governance of Estonia. What can we really learn from that pairing? So this week, I want to spotlight the Singapore of Africa. A country that made remarkable progress amidst a backdrop of conflict (read: genocide): reducing their U5MR nearly 6-fold in 30 years. Let’s dive into Rwanda, famously known in the global health circles as an exemplar on the topic.
Global U5MR decline
As you (now?) know, the U5MR is essentially made up of 2 components: the neonatal mortality rate (deaths within the first month) and the 1-59 months mortality rate. This distinction is important, because more than 1 in 3 global deaths under-five are due to neonatal conditions:
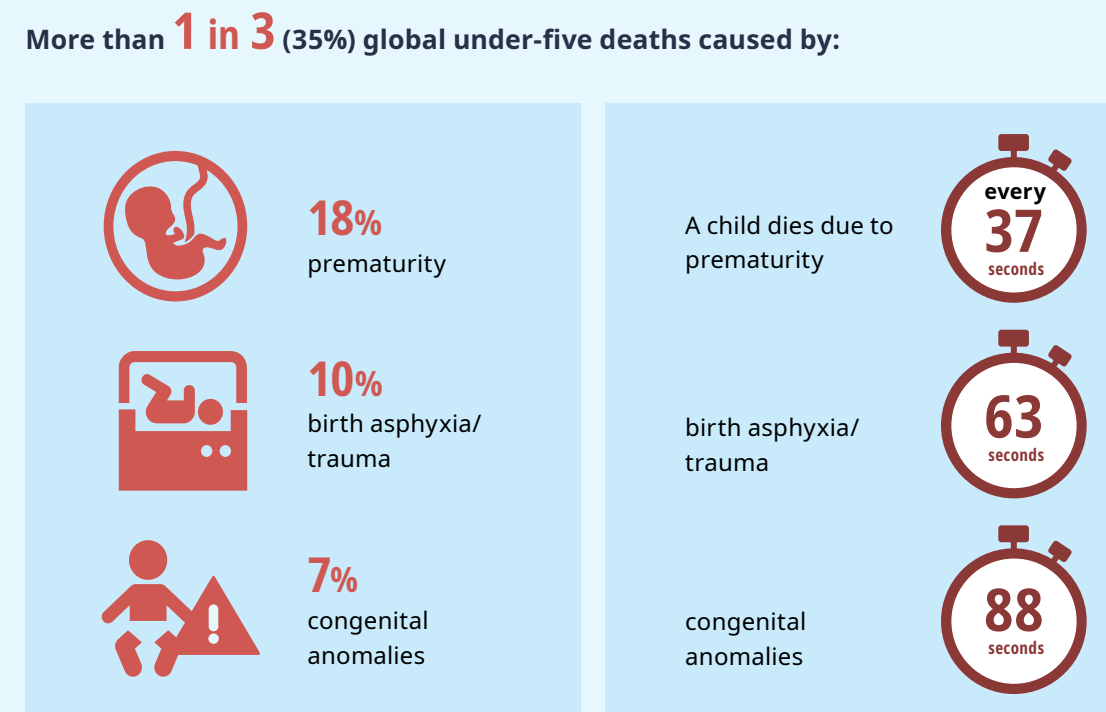
Source: United Nations Inter-agency Group for Child Mortality Estimation (UN IGME), Levels & Trends in Child Mortality: Report 2025
As recently as two centuries ago, around 1 in 2 children died before reaching the end of puberty. Reduction in U5MR globally has been one of the biggest (recent!) success stories in global health, and has taken place across every single region of the world. This is thanks to simple innovations and medicines that are effective (and cheap!), vaccinations, improved sanitation, and access to family planning. You can read this short note from Bill Gates from a few years ago (someone whose passion for global health and development reportedly started with U5MR) where he explores some life-saving innovations that result in: stopping women from bleeding to death after childbirth, preventing life threatening infections during labor, speeding the development of babies’ lungs, fighting malnutrition before and after birth, and more.
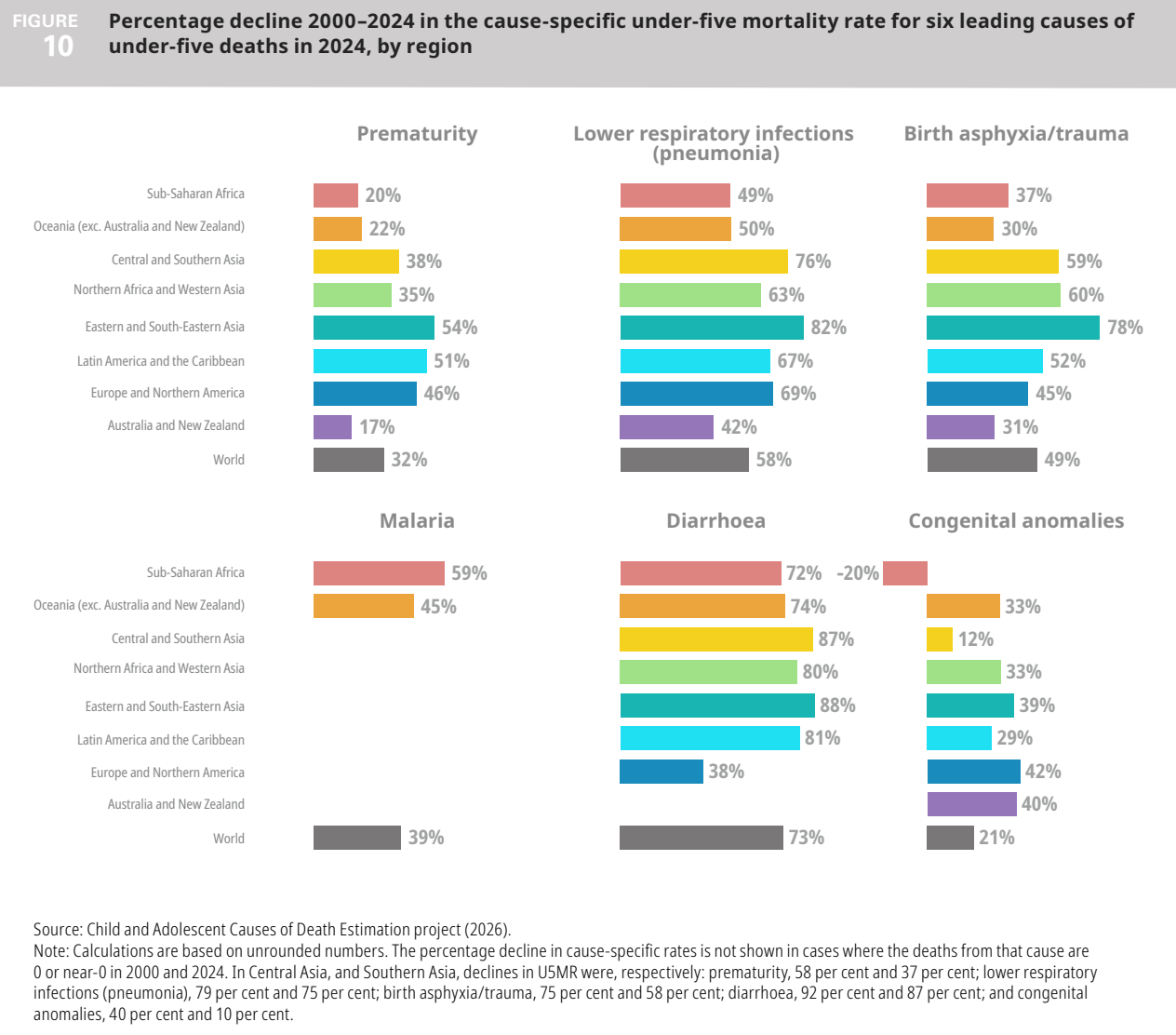
There has been steady progress in reducing deaths from the six leading causes of U-5 deaths in every region, see below. This is, to be very honest, thrilling.
That said, whether that progress is going to be sustained from 2024 onward is an open question. Due to the decimation of foreign assistance from the US and other governments, the future is uncertain. The Gates Foundation’s 2025 Goalkeepers Report estimates that a 20% reduction in development assistance for health funding from 2024 levels would result in 12 million more children dying by 2045 and 16 million more if cuts are even steeper at 30%. The Rwandan health system needs external financing - PEPFAR, Global Fund, etc (including for the Mutelles program which I explore more below), and more. It now all stands to be tested.
U5MR in Rwanda
These are largely preventable deaths. Because we know what works, because we have seen it in countries across the world, especially in Rwanda. Look at this astonishing figure below from the Rwandan census (IMR = infant mortality rate, i.e. the first year of life, CM = age 1-4). The period of conflict resulting in genocide was between 1990-94. If you look at the green line (U5MR), you see that in 2002, it was at 227 deaths (per 1,000 live births). To put that in context, recall that our current highest U5MR country, South Sudan, is at roughly 100 now.
Rwanda’s progress was remarkable. The U5MR dropped from 227 to 72 in 2012, continuing to drop further to 41 by 2022. It is currently lower still, at 36 according to the 2025 DHS.
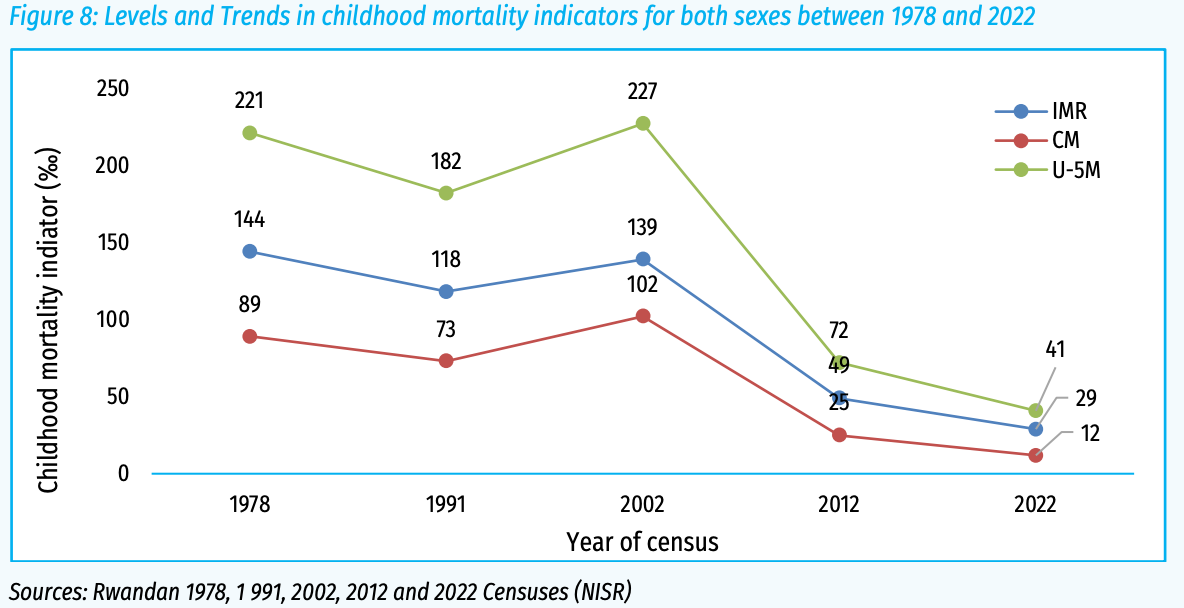
Source: Statistics Rwanda (2025)
Other indicators from the recently concluded DHS also show steady (and dramatic) progress that is related to the trendline above:
Total Fertility Rate (TFR) went down from 6.1 in 2005 to 3.7 in 2025; use of modern contraception increased from 10% to 64% in that same time period;
95% of women receive antenatal care from a skilled provider (essential to monitor pregnancy and reduce morbidity and mortality risks for the mother and child);
92% of women took iron-containing supplements during pregnancy;
98% of births were delivered by a skilled health provider;
78% of women received sufficient doses of tetanus diphtheria to safeguard their last live birth against neonatal tetanus and diphtheria;
68% of women had a postnatal check during the first 2 days after birth;
94% of children aged 12-23 months are fully vaccinated with basic antigens (BCG, 3 doses of polio and DPT, single dose of measles vaccine);
The proportion of children that were stunted decreased from nearly half in 2000 to 27% today; the proportion underweight decreased from 20% to 6% in the same time period.
I could go on. The point is that Rwanda has made exceptional progress across health indicators. It does all that with actual spending on health quite low. Would you believe that it spends less than South Sudan on health (as a % of GDP), at 5% compared to 11%? It speaks to the efficiency of the spend, and the impact of foreign assistance on the overall health budget.
Here are a few factors that stand out to me regarding Rwanda’s U5MR story.
Imihigo
In Rwanda, every district mayor signs an annual contract with the President, in public, on television (if I am not mistaken), listing what they will deliver to their constituents. The word, imihigo, is roughly translated into a vow or a pledge. The synopsis below is super helpful, you can read the full article if interested:
In the wake of the 1994 genocide, the Rwandan Patriotic Front (RPF) inherited the remnants of a highly centralized state administration. For a number of years the government engaged in crisis management, attempting to meet the basic needs of a traumatized population. In 2000, in an effort to improve local service delivery, the RPF-led government began a program of decentralization. Under the new arrangement, mayors were responsible for implementing development programs. A chief concern for the central government was how to make mayors accountable. In response to this challenge, the government in 2006 launched an innovative system known as the imihigo process. Imihigo had its roots in a pre-colonial Rwandan cultural practice whereby leaders or warriors would publicly vow to achieve certain goals—and face public humiliation if they failed. The modern imihigo process linked this traditional Rwandan practice with planning, monitoring and oversight.
Princeton publication (2011)
By 2010, imihigo had come to refer to a combined performance-management system, planning tool, multi-layered oversight mechanism, and way of using social and traditional pressure to push mayors to greater levels of achievement. Annual report cards help with accountability and likely, public naming and shaming of underperforming areas. While designed to be decentralized, it really is a structure aimed at providing feedback to the central government. Keep in mind also that according to Freedom House:
The Rwandan Patriotic Front (RPF), led by President Paul Kagame, has ruled the country since it ousted forces responsible for the 1994 genocide, ending the civil war that began in 1990. While the regime has maintained stability and economic growth, it has also suppressed political dissent through pervasive surveillance, intimidation, arbitrary detention, torture, and renditions or suspected assassinations of exiled dissidents.
Indeed, while the idea of imihigo is polarizing, there is some research to show that it helped improve the rates I showed earlier and others - vaccinations, stunting reduction, facility delivery rate, latrine coverage etc. It has also been credited with driving high nationwide health insurance coverage (exceeding 90%), called Mutuelle de Santé (there’s a USAID connection, see prior link), and accelerating the construction of health centers. Specific to child survival, Rwanda achieved a 74% reduction in under-5 mortality (U5M) between 2000 and 2015, particularly improvement in neonatal survival thanks to skilled birth attendants at time of delivery. This success was supported by the implementation of evidence-based interventions (EBIs) such as vaccinations (pentavalent and rotavirus), facility-based delivery, and integrated management of childhood illness. During the COVID-19 pandemic, the Imihigo framework and the existing culture of accountability helped ensure that essential maternal and child health services were prioritized and maintained, despite initial moderate drops in vaccine administration and facility-based deliveries.
The level of coordination that is involved in this system likely boosts the use of data in planning and implementation, and allows the central government to guide donor funding toward actual specific needs of the country, rather than vertical silos of donor prioritization. This ensures that foreign aid is aligned with Rwanda’s priorities, and not any other way.
Umuganda
In addition to imihigo, Rwanda draws on a number of additional traditional practices to bolster decentralization efforts at the local level. One of these is umuganda, basically a monthly community work project like planting trees and repairing bridges and roads, and cleanliness. NPR did a great piece on it a few years ago, here, which traces the dark history of the word to what it means today and controversies. According to a WHO report, Umuganda is a good opportunity for health promotion and behaviour change communication where the messages regarding malaria prevention, hygiene and sanitation, Community Based Health Insurance adherence, fight against malnutrition etc are provided. I can’t find researchy-research to link this practice directly to lower U5MR, but much like my non-research driven consensus from last week that leaving babies outside to nap in the freezing cold is probably a good thing, holds. Related, in 2008 Rwanda became one of the first countries in the world to ban single-use plastic bags and bottles; it is now a global leader (along with Norway) in a coalition to develop a global treaty to end plastic pollution by 2040. The health implications of plastic pollution are alarming, and relate to U5MR generally speaking:
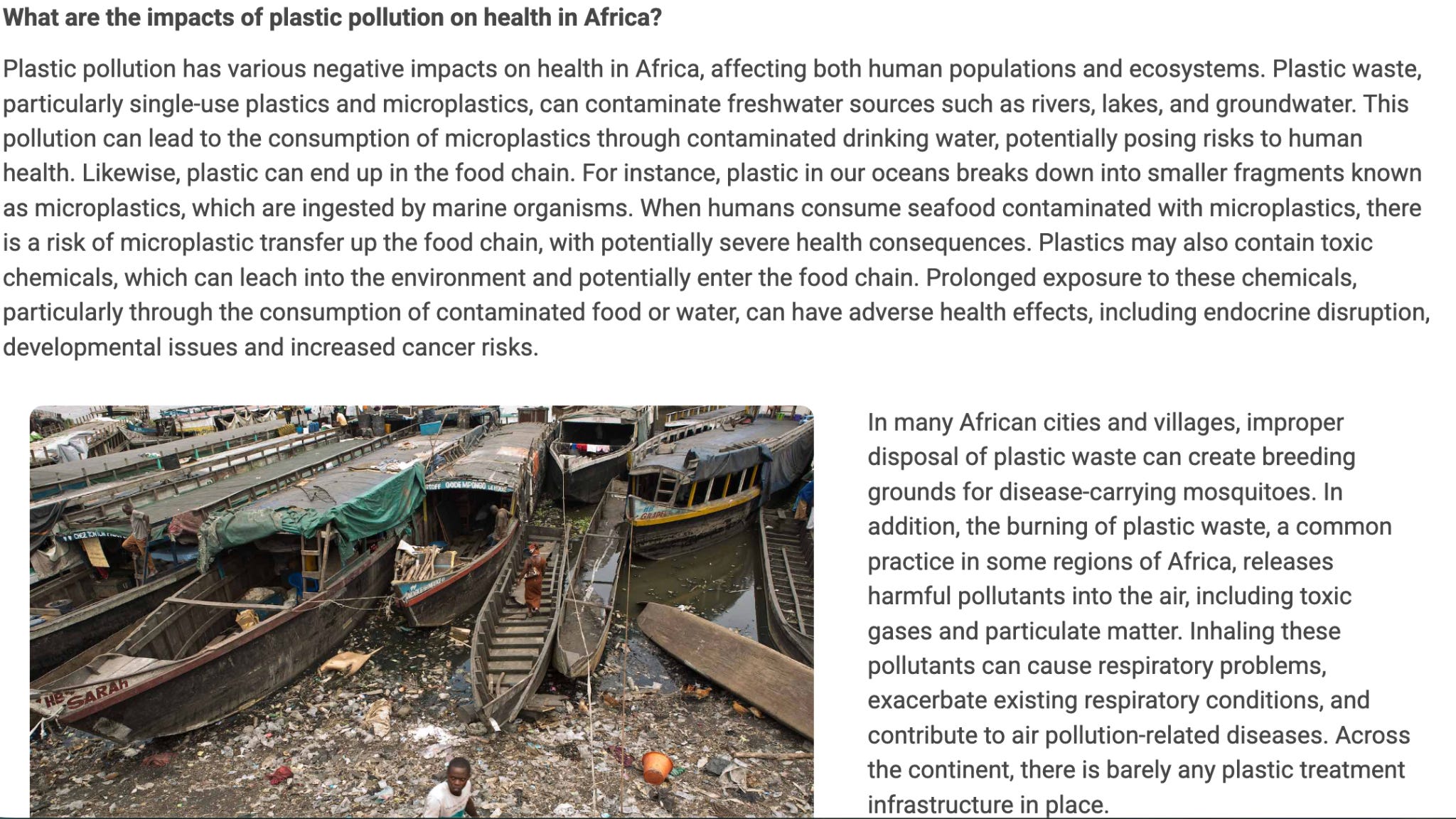
Source: WHO (2023)
Binômes
Much like lady health workers we saw in other pieces (Pakistan, Iran to name a few), Rwanda has its own thing. It has one community health worker (Assistante Maternelle de Santé ) and one binôme (a paired man and woman) per village of approximately 50 to 150 households. These CHWs are trained for about 3 months, and focus on health promotion and providing referrals to clinics. They are elected by their neighbours, and provide a spectrum of services: health promotion and prevention; integrated community case management of childhood illness; maternal and newborn health; identification of TB suspects and referral and community TB DOTs; community based distribution of family planning; nutrition.
CHWs have significantly contributed to the transformation of Rwanda’s health system and remain key to advancing universal health coverage. For 30 years, Rwanda’s CHW programme has improved maternal and child health and proven vital in managing outbreaks. You can read the Exemplars report if you are curious about the magnitude of specific interventions that curbed U5MR. Most of them are driven by the CHW engine. They are likely also responsible for the gap closing dramatically between the best and worst performing districts in the country. The worst-performing districts get supplementary support rather than budget cuts.
But, they are not paid; they are incentivized through two methods of community performance based financing (C-PBF). Essentially, the first is based on CHW ooperative-level achievement of specified targets, and the second on individual event-based reporting through a RapidSMS program for cell phones. Anecdotally, CHWs take home around US$ 5 to US$ 10 on a quarterly basis. Their performance bonus is tied to facility-level Imihigo outcomes, and they belong to cooperative income-generating activities that channel state subsidies.
While the outcomes are amazing, you can guess that all is not always rosy:
CHWs report heavy paperwork burdens, logistical constraints such as inadequate transportation support, stock outs of essential supplies. Workload overload, compounded by expanding responsibilities, threatens CHWs’ capacity to maintain quality and enthusiasm. These systemic challenges are consistent with global evidence on CHP emphasising the urgent need for digital health solutions, logistical support and systemic reforms to streamline reporting and supply chains.
Now think about the e-health system in Estonia and how amazing it would be to get close to that in Rwanda. Honestly, if any country can do it, it’s like them.
The return of doctors
In the Nigeria piece, we talked about the brain drain, specifically of healthcare workers and doctors. Without skilled professionals, already strained systems teeter precariously which shows up in health outcome data. Well, between 2024 and 2028, Rwanda aims to quadruple its health workforce, already starting out strong.
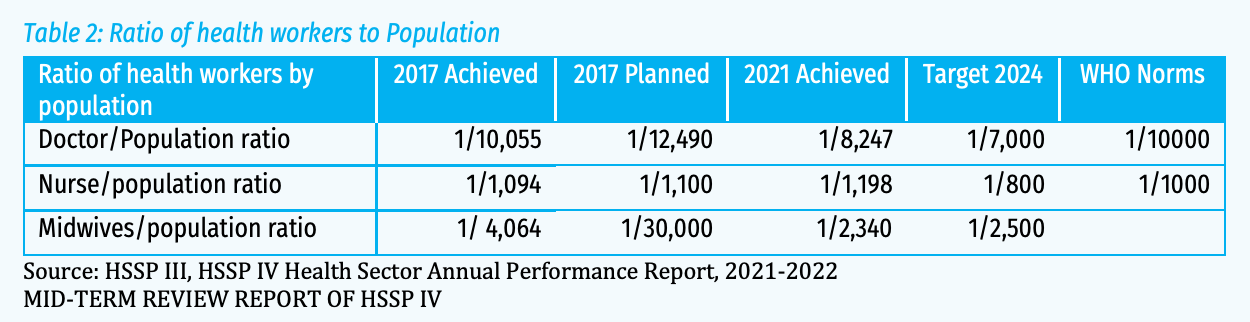
Source: Statistics Rwanda
A study by the Center for Global Development reviewing census records showed that due to the war, Rwanda lost almost 43% of its medical workforce to other countries between 1999 and 2001. Now, almost all doctors that leave Rwanda for specialized training return to work in Rwanda. According to experts, this is due to three main reasons:
First is the fairness of the system in according whoever is competent an opportunity to specialise. Whereas in some countries, you need to be well ‘connected’ to access these scholarships, in Rwanda the system is driven by merit. Therefore, because of these opportunities of continuous professional development, Rwanda’s medics feel indebted to serve their country.
Secondly and most important, though our health professionals are relatively remunerated well, compared with their colleagues in the region, their motivation is not necessarily money driven but rather derived from working in an environment that is progressive.
Source: Center for Global Development (2012)
One other factor identified by the Africa CDC:
Fostering a strong sense of national duty among those who study overseas, encouraging them to return and contribute to the country’s development.
Source: Africa CDC (2025)
Doctors, midwives, nurses working in concert with CHWs seems like the dream, and no doubt contributes massively to the gains in U5MR, life expectancy, and so much more.
When women are in government
Rwanda has consistently led the world in female parliamentary representation. The new constitution in 2003 introduced a 30% gender quota for all elected positions in government. This policy aimed to promote gender equality and increase women’s representation in decision-making roles. The mandate paved the way for significant reforms led by women parliamentarians such as equal access to land ownership and labor laws for equal pay. Since then, this threshold has been regularly − and widely − exceeded in Parliament - it stands at 59% in the national legislature currently and at 46% in local legislature.
This matters for so much. The Council on Foreign Relations’ Women’s Power Index indicates that women’s leadership promotes cooperative governance and peacemaking, democracy, social welfare, equality, and economic progress. When women make up a critical mass in legislatures—around 30%—they are more likely to achieve those goals in spending and policy agendas, likely by allying with other women.
I am shameless and will plug this piece I co-wrote recently for Think Global Health to give you a full picture of what I mean for health and U5MR specifically:
Research suggests that electing women leaders could lead to improved health outcomes. A global assessment conducted between 1990 and 2020 found that women’s political representation correlates with decreases in maternal mortality and better child-health outcomes, particularly in South Asia and sub-Saharan Africa. Countries have achieved success through substantive representation: women legislators are more likely to sponsor and pass bills related to sexual and reproductive health rights, which directly impact maternal survival. The introduction of gender quotas in parliaments led to a 9% to 12% decline in maternal mortality, driven by increases in skilled birth attendance and prenatal care utilization. Increasing the proportion of women in national legislatures has been demonstrated to similarly reduce epidemic-related mortality. Women are likelier to prioritize public health and to advocate for investments in health infrastructure.
Source: Think Global Health (2026)
In Rwanda, research indicates that women parliamentarians have become strong advocates for children and families, initiating pro-child legislation and prioritizing children’s needs in the national budget.
Looking ahead
I read 2 papers in the last week that got me thinking about Rwanda’s progress and what’s next on the horizon in a different context. We discussed the obvious open question - that of foreign assistance. The next frontier of Rwanda’s demographic success will be defined by its ability to insulate health gains from an increasingly volatile environment. [Side note: Rwanda’s climate change data portal is amazing.] While the nation has built a world-class community engine of binômes and achieved remarkable stability in its medical workforce, the structural mechanics of survival are shifting. This paper from Nature suggests that the physical geography of healthcare is under threat in analysis from 21 countries in sub-Saharan Africa: extreme precipitation events lead to tens of thousands of births occurring outside the safety of health facilities because the weather makes travel to health facilities impossible.
Look at this trendline which shows the increase in births that took place at a health facility, or were from a skilled provider in Rwanda. Access to proper medical attention and hygienic conditions during delivery can rescue the risk of complications and infections that may lead to death or serious illness for mom and/or baby.
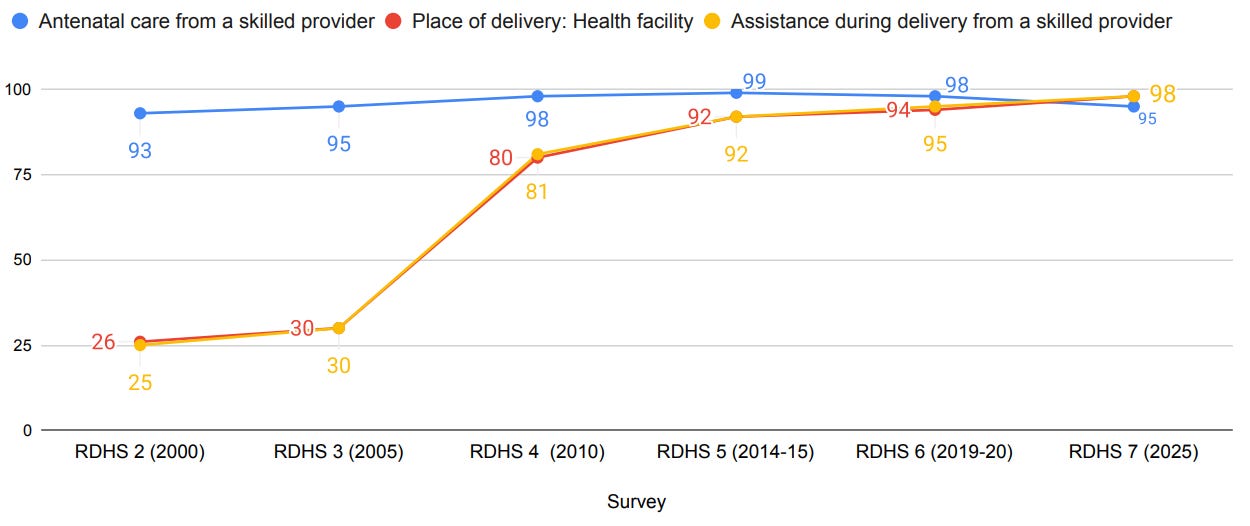
The paper I mentioned shows that each additional day of heavy rainfall in the 3 days before birth is linked to about 11 more live births per 1,000 happening outside a health facility. One of the main reasons why neonatal mortality improved over time in Rwanda, was that births were happening in health facilities. If climate pressures now make getting to health facilities harder still, it’s likely to affect this trendline.
Rwanda made enormous strides in improving nutrition for children (recall the stunting data). One thing I didn’t mention yet but is lovely so I have to: Cows play an important role in Rwanda, much like the cow economy in South Sudan. While the latter model is an ancient survival strategy currently strained by conflict and climate change, the Rwandan model is a deliberate policy tool designed to use the cow as a lever for poverty reduction and pediatric health. Here is how it works: In 2006, the Rwandan government set up a program aimed at cutting poverty and improving health and nutrition in rural areas by providing a cow per poor family. The idea was simple: given a cow, a poor family suddenly has milk to drink and manure with which to fertilize crops. As of 10 years ago, more than 130,000 cows have been distributed through the program, which goes by the name Girinka. When the cow gives birth to a female calf, the family must give that calf to a neighbor. Research shows that the program has a positive effect on the value of per hectare crop production, indicating that the livestock has enabled households to improve their agricultural productivity. Crucial for our story, the available evidence suggests that this program increased household income through the sale of milk and because fertilization of soils with manure has also raised crop yields. Girinka appears to have helped cut malnutrition rates as well.
Looking ahead, the challenge is not just whether there will be enough food, but whether that food still possesses the power to nourish. This paper finds that rising atmospheric CO2 is fundamentally altering the chemistry of global staples, triggering a dilution effect where crops grow larger but lose critical concentrations of protein, iron, and zinc. This represents a hidden tax on future development. Even if children survive those critical first 5 years, poor nutrition would affect their overall health and development.
To remain an exemplar, Rwanda’s next Imihigo must bridge this gap, integrating climate adaptation and nutrient security into the very heart of maternal and child health policy.
The Food!
I couldn’t decide whether to make agatoto or igisafulya, so I ended up making a mashup of both (sorry!) It was delicious, and we ate it with ugali which the kids enjoyed playing with, sweet potatoes (random, but I felt like it), and kachumbari on the side. This week, Eymir did not slack off - he presented on the geography and history of the country while Kimaya did an interpretive dance to music from Andy Bumuntu.